How is Structural Compromise Assessed?
Structural compromise is assessed by checking the tooth for 4 red flags, and also by taking a detailed history from the patient.
What are the 4 Red Flags?
- Cracks into dentin
- Isthmus width > 2 mm
- Cusp thickness < 3 mm
- Box depth > 4 mm
1) Cracks into dentin
Cracks into dentin can sometimes be visualised as Peripheral Rim Fractures (PRF). In order to determine if a PRF extends into dentin, the patient’s history (e.g. sensitivity to cold/sweet or pain on biting) and overall assessment of structural compromise must be taken into account.

Photo credit: Dr Pete Butkus
2) Isthmus width > 2 mm
In 1981, Larson, Douglas, and Geistfeld analysed the effect of cavity preparation on the strength of teeth. They found that creating an isthmus width of 1.5 mm resulted in a 40% reduction in fracture resistance. By creating an isthmus width of 2 mm, the fracture resistance was reduced by 60%.
Similarly, Magne and Oganesyan carried out a finite element analysis study of cuspal deflection following operative procedures in 2009. Their study compared the micromovement of unbonded restorations and bonded restorations. The following results were obtained in terms of the micromovement of cusps:
- No cavity prepared – 2.7 microns
- MOD cavity unbonded – Up to 180 microns
- MOD cavity restored using composite – 6.9 microns
An amalgam restoration or unbonded composite restoration can cause the tooth to be flexing in a non-biomimetic way, leading to further caries and fracture.

Photo credit: Dr Pete Butkus
3) Cusp thickness < 3 mm
A cusp which measures less than 3 mm in thickness is considered a “dry” cusp. The cusp is no longer hydrated as the connection between the pulp and DEJ via the dentinal fluid is lost. A “dry” cusp measuring less than 3 mm in thickness can flex 3x as much as a hydrated cusp.

Photo credit: Dr Pete Butkus
4) Box depth > 4 mm
A box depth of 4 mm (measured vertically from the marginal ridge of the adjacent tooth) extends into the BioRim of the tooth. Beyond 4 mm, enamel in the BioRim region is decussated, meaning that the prisms are irregularly arranged and are not in a normal configuration. Enamel in this region should not be beveled as a uniform bevel cannot be achieved – a butt margin should be used. This concept is discussed further in Lesson 5 of the SLA to BRD.
If the BioRim has been lost, it can be restored using Deep Margin Elevation (DME). Optimal stress-reducing protocols are required in these areas.
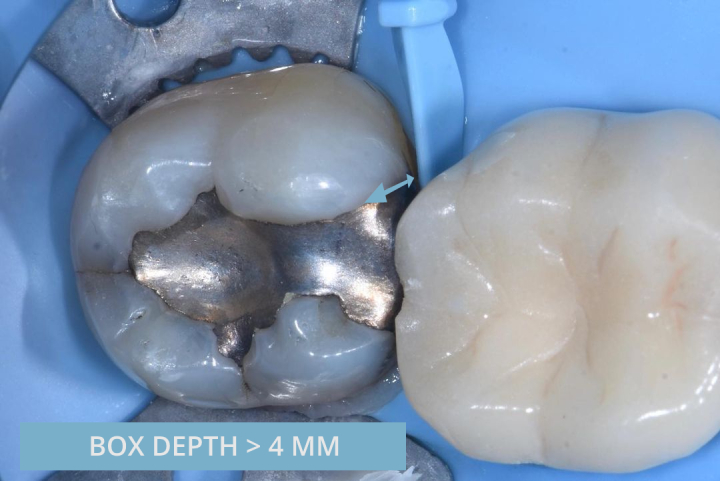
Photo credit: Dr Pete Butkus
The Rainey Ridge & Peripheral Rim Fractures (PRF)
The sub-occlusal oblique transverse ridge (also known as Rainey Ridge) is a structure which runs underneath the pits and fissures of the tooth, helping to connect the tooth together side to side; front to back; and top to bottom.
If a traditional cavity preparation is carried out and these ridges are cut, the tooth is no longer connected in a biomimetic way. The tooth is now able to open and close and can flex in a range of around 200 microns. This can result in stress concentration. Fracture resistance decreases and the marginal ridges are more likely to crack, leading to Peripheral Rim Fractures (PRF).
Crack Propagation
Cracks can propagate when under occlusal loading. As discussed previously, teeth will generally bend and flex, and will fatigue over time before eventually fracturing. A small crack requires more force to be applied in order to propagate. Longer cracks require less force to be applied before propagation occurs.
After carrying out structural analysis using the 4 red flags method, take a thorough history to determine if the patient has had any sensitivity to cold, sweet, or when biting. Also check if the patient has had any symptoms in the past. As written by Brannstrom in 1986, remineralisation of the cracks can result in temporary relief of symptoms due to tertiary dentin formation and reduction in hydrodynamic movement. This can make diagnosis of cracked tooth syndrome very difficult.
Managing Cracks
Cracks into enamel may be considered biomimetic, as by restoring the tooth back together adhesively, the resulting flexure of the tooth is unlikely to cause catastrophic fracture or secondary caries. Cracks into dentin, however, cannot be considered biomimetic and should be dissected where possible.
Techniques such as providing full coverage crowns, partial onlays, carrying out occlusal adjustment or simply bonding over cracks using composite or fibre such as Ribbond, are unlikely to be successful in these situations. This is because the crack is still present, and the crack can therefore still continue to propagate. Providing partial coverage onlays or attempting to bond over horizontal or oblique cracks may provide some initial benefit, but this method is unlikely to be successful for vertical cracks.
Oblique/horizontal cracks are less likely to lead to pulpal death. If these are not identified then the most common sequelae would be cuspal fracture. Vertical cracks are more likely to lead to pulpal death or catastrophic fracture.
Crack dissection should be considered as the technique of choice.
Crack Visualisation
As with all techniques, high magnification is strongly recommended.
Old cracks are likely to stain darker and can therefore be identified more easily. Newly formed cracks are usually lighter in appearance, and can therefore be more difficult to visualise. If onlaying a thin cusp is appropriate (as per Lesson 5) then this may help with crack visualisation.
Visualisation by Crack Dehydration
When assessing an oblique or horizontal crack, it can be difficult to distinguish any notable difference in opacity without drying the tooth. After air drying the tooth for 10 seconds, the dentin above the crack will appear more opaque as it receives less hydration from the pulp. In relation to vertical cracks, each side of the crack receives similar levels of hydration from the pulp, and therefore alternative techniques should be considered.
Visualisation by use of Primer
Applying a layer of primer can alter the light refraction of the crack. This can allow better visualisation.
Dissection of Cracks and Crack Removal Endpoints (CrRE)
If it is necessary to remove a restoration in order to assess for cracks, or if cracks are encountered during an operative procedure, crack dissection should be carried out and Crack Removal Endpoints (CrRE) should be followed. The aim is to remove cracks without exposing the pulp. Measurements of 3 mm horizontally from the adjacent tooth’s marginal ridge and 5 mm vertically from the cavity margin are used. Crack removal is halted at this point, in a similar way to the Caries Removal Endpoints (CRE) in order to achieve a Peripheral Seal Zone (PSZ) free from cracks. The area over the pulp, encircled by the PSZ, is commonly referred to as the Central Stop Zone (CSZ).
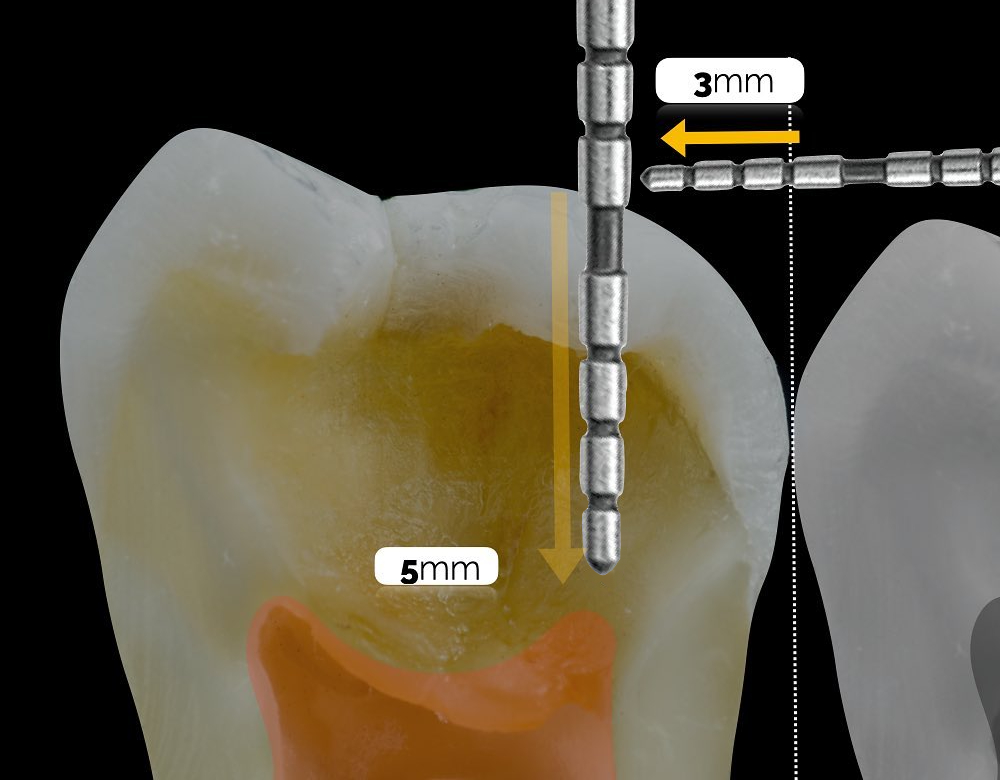
Photo Credit: Dr Andres Celi
The aim of crack dissection is to remove the crack in order to prevent future crack propagation. The technique is based on engineering principles. Complete crack removal in the PSZ is aimed for. If partial crack removal is achieved then there is a chance that the crack will continue to propagate, however as the lever arm of the crack has been shortened, greater force is required to cause crack propagation. Perforation or pulpal exposure should be avoided.
If partial crack removal is carried out in the Central Stop Zone (CSZ), placement of Ribbond (leno woven ultra high modulus polyethylene fibre) is recommended within the Biobase (see Lesson 3). This can help to reduce stress concentration at the crack interface by redirecting forces.
Restoration of the dissected crack should be carried out using the principles of Lesson 3 and Lesson 4. This commonly involves applying layers of Immediate Dentin Sealing (IDS) and Resin Coating (RC) as normal, followed by restoration with thin horizontal layers of composite resin. AP-X (dentin-replacing composite) or EverX Posterior (Short Fibre-Reinforced Composite) are commonly used in small 1 mm increments. Restoring crack dissections is very challenging due to the high C-Factor environments encountered.
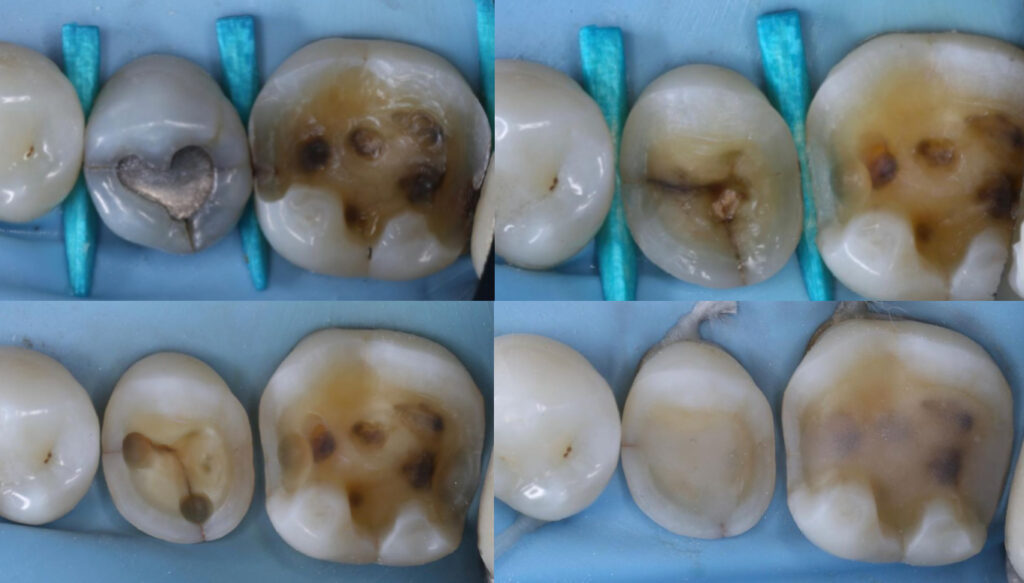
Photo credit: Dr Matt Penz
Occlusal Effect Caries (OEC)
Occlusal Effect Caries (OEC) is caries that forms as a result of biofilm formation inside cracks. These cracks are commonly a result of Peripheral Rim Fractures (PRF). Bacteria enters through the PRF which is located on the occlusal aspect of the tooth. This type of caries can be more difficult to detect on radiographs, as the typical interproximal radiographic appearance will likely not be present. The following clinical example of OEC has been kindly provided by Dr Ashley Chung.
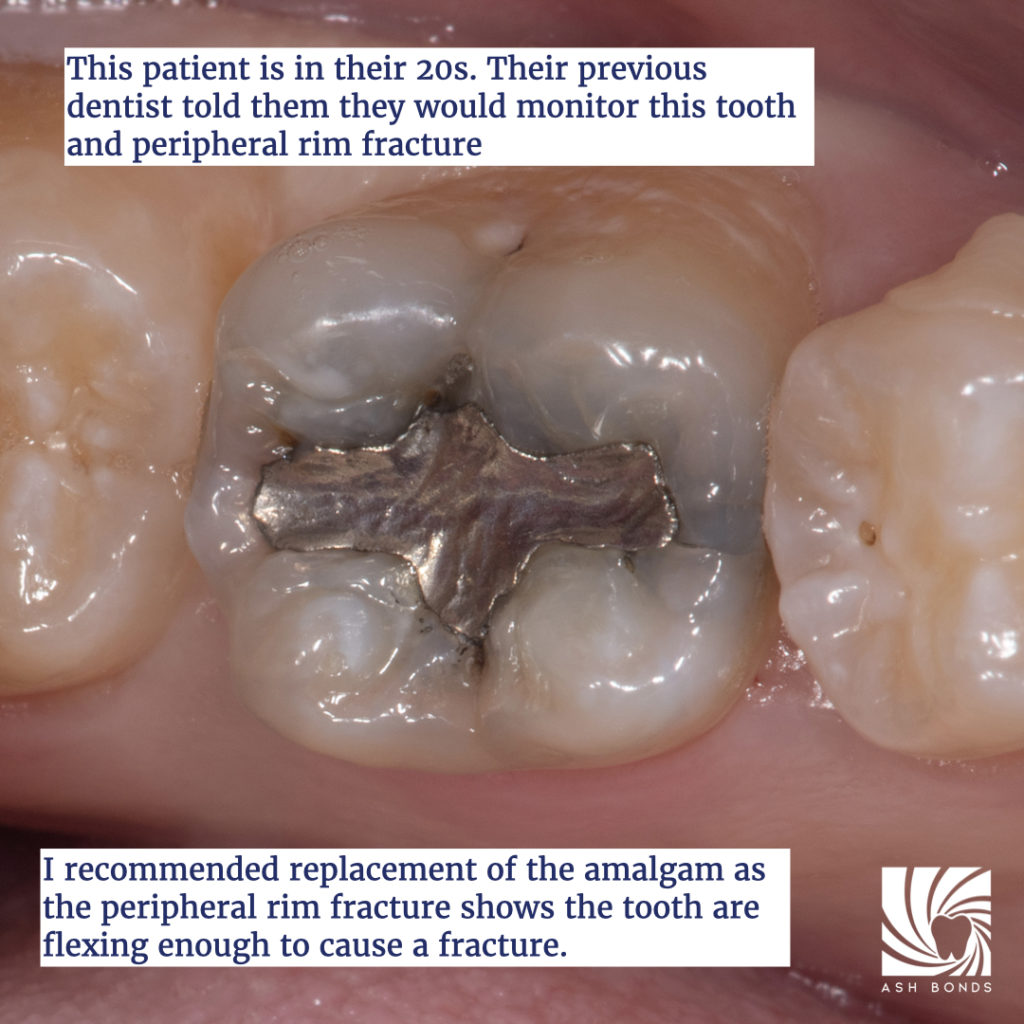
Photo credit: Dr Ashley Chung

Photo credit: Dr Ashley Chung
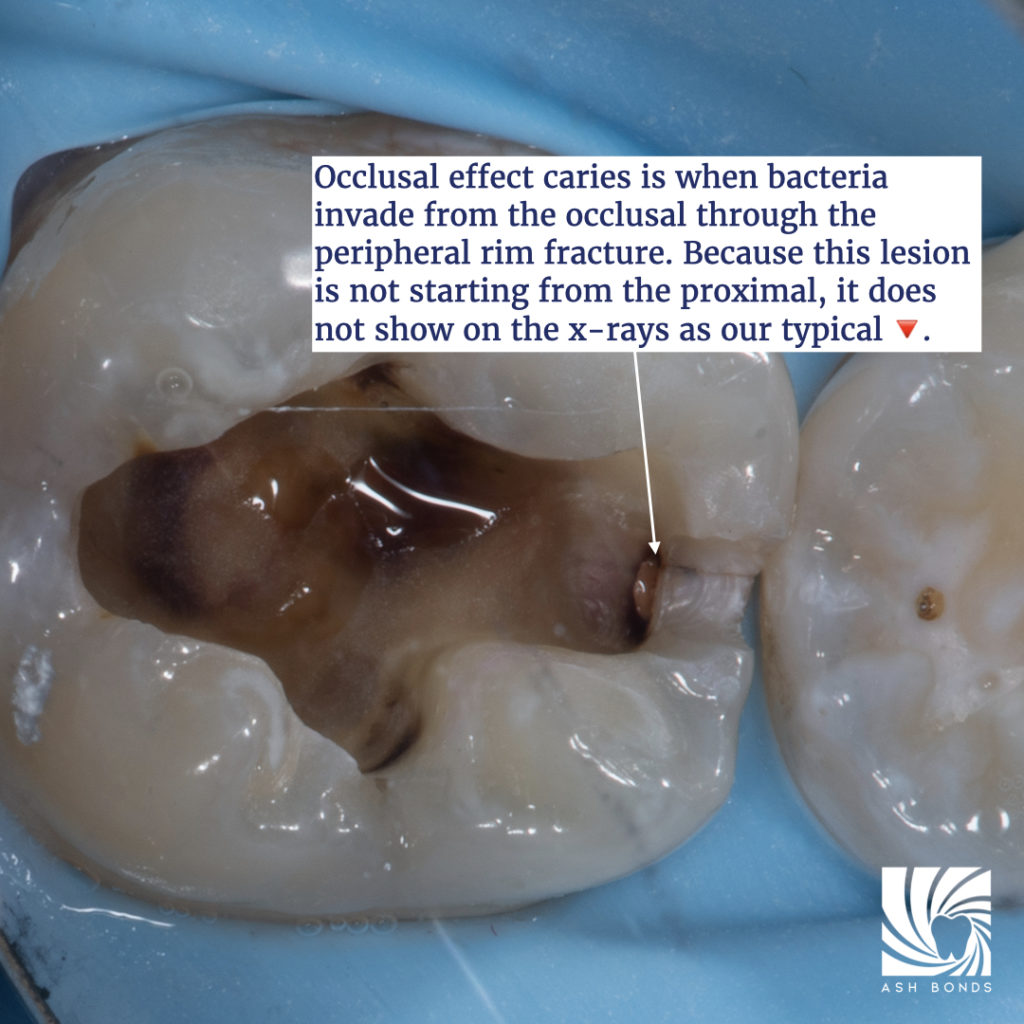
Photo credit: Dr Ashley Chung
Relevant Literature
Belli S, Erdemir A, Ozcopur M, Eskitascioglu G. The effect of fibre insertion on fracture resistance of root filled molar teeth with MOD preparations restored with composite. Int Endod J. 2005 Feb;38(2):73-80.
Brannstrom M. The hydrodynamic theory of dentinal pain: sensation in preparations, caries, and the dentinal crack syndrome. J Endod. 1986 Oct;12(10):453-7.
Kishen A, Vedantam S. Hydromechanics in dentine: role of dentinal tubules and hydrostatic pressure on mechanical stress-strain distribution. Dent Mater. 2007 Oct;23(10):1296-306.
Krell KV, Rivera EM. A six year evaluation of cracked teeth diagnosed with reversible pulpitis: treatment and prognosis. J Endod. 2007 Dec;33(12):1405-7.
Larson TD, Douglas WH, Geistfeld RE. Effect of prepared cavities on the strength of teeth. Oper Dent. 1981;6(1):2-5.
Magne P, Boff LL, Oderich E, Cardoso AC. Computer-aided-design/computer-assisted-manufactured adhesive restoration of molars with a compromised cusp: effect of fiber-reinforced immediate dentin sealing and cusp overlap on fatigue strength. J Esthet Restor Dent. 2012 Apr;24(2):135-46.
Magne P, Oganesyan T. CT scan-based finite element analysis of premolar cuspal deflection following operative procedures. Int J Periodontics Restorative Dent. 2009 Aug;29(4):361-9.
Milicich G, Rainey JT. Clinical presentations of stress distribution in teeth and the significance in operative dentistry. Pract Periodontics Aesthet Dent. 2000 Sep;12(7):695-700.
Opdam NJ, Roeters JM. The effectiveness of bonded composite restorations in the treatment of painful, cracked teeth: six-month clinical evaluation. Oper Dent. 2003 Jul-Aug;28(4):327-33.
Opdam NJ, Roeters JJ, Kuijs R, Burgersdijk RC. Necessity of bevels for box only Class II composite restorations. J Prosthet Dent. 1998 Sep;80(3):274-9.
Opdam NJ, Roeters JJ, Loomans BA, Bronkhorst EM. Seven-year clinical evaluation of painful cracked teeth restored with a direct composite restoration. J Endod. 2008 Jul;34(7):808-11.
Politano G, Van Meerbeek B, Peumans M. Nonretentive Bonded Ceramic Partial Crowns: Concept and Simplified Protocol for Long-lasting Dental Restorations. J Adhes Dent. 2018;20(6):495-510.
Rainey JT. A sub-occlusal oblique transverse ridge: identification of a previously unreported tooth structure: the Rainey Ridge. J Clin Pediatr Dent. 1996 Fall;21(1):9-13.
Ratcliff S, Becker IM, Quinn L. Type and incidence of cracks in posterior teeth. J Prosthet Dent. 2001 Aug;86(2):168-72.