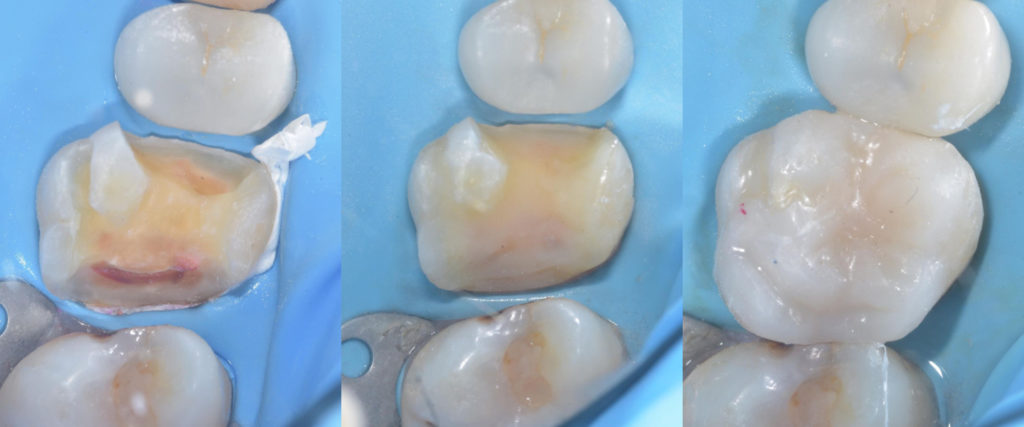
From left to right: (1) CRE and PSZ established. (2) Biobase created. (3) Final restoration.
Photo Credit: Dr Davey Alleman
Lesson 5 of the Six Lessons Approach to Biomimetic Dentistry relates to preparation design (e.g. onlay, overlay) with an adhesive restoration in mind. The fifth lesson also covers preparation and bonding to enamel.
Enamel Rod/Prism Orientation
The tensile strength of enamel is dependant on the orientation of the enamel rods or prisms. The study by Carvalho et al. in 2000 found that the tensile strength of enamel with prisms positioned parallel to an applied load was 24.7 MPa. With a perpendicular load applied to the enamel prisms, the tensile strength was found to be 11.4 MPa.
Master Biomimetic Dentistry Online.
Increase predictability. Reduce stress.
Davey Alleman, DMD
Beveling Enamel
Appropriate beveling can help to prevent separation of the enamel at the orientation lines of the rods/prisms.
There are several methods of beveling enamel e.g. by using finishing burs. Another system available is the Sonicsys by Kavo which contains a smooth side and a diamond side, with a vibrating tip.
Bevel or Butt Joint?
Gingival enamel should only be beveled if:
- It is thicker than 1.5 mm
- Box depth is less than 4 mm.
If the enamel is thinner than 1.5 mm or the box depth is >4 mm, then a butt joint should be opted for. This is because the enamel in this region is decussated, meaning it has an irregular orientation and a uniform bevel cannot be achieved. This concept is also explored in the structural analysis stage of Lesson 2 of the SLA to BRD.
Cusp Thickness and Occlusal Reduction
The cusp thickness should be measured from the base of the cusp using callipers. It is commonly recommended that holding (functional) cusps <2 mm and tension (non-functional) cusps <3 mm should be onlayed. Depth grooves should be created of known depth (2-3 mm), and these grooves should then be connected using a straight diamond bur.
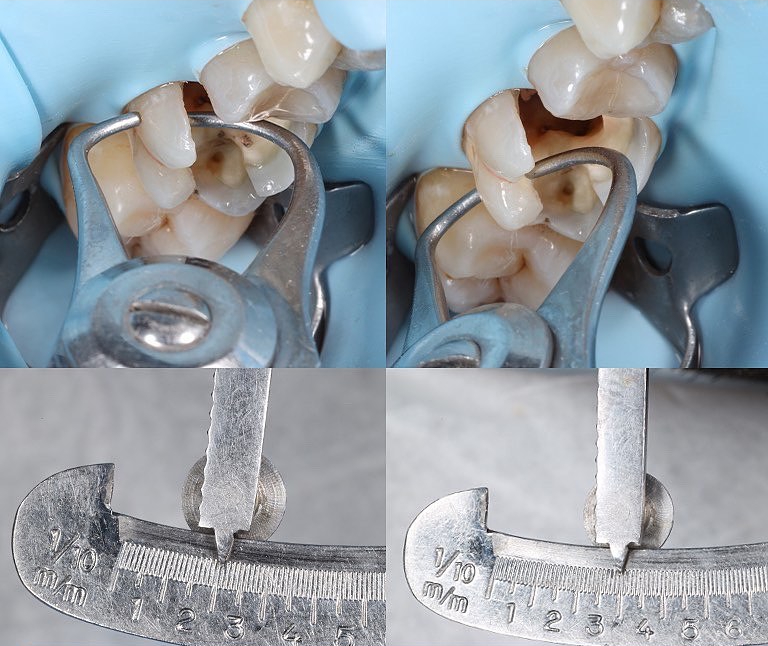
Photo Credit: Dr Péter Farkas
This also contributes to reduction of C-Factor as explained in Lesson 4.
The holding/functional cusps (palatal cusps of the upper teeth and buccal cusps of lowers) should be preserved where possible, as long as the thickness at the base of the cusp is at least 2 mm.
Optimum stress-reduced techniques (e.g. the “wallpapering” technique if the final restoration is a Stress Reduced Direct Composite) can be used in some cases to reduce the cusp thickness below even 2 mm.
A hollow chamfer can be beneficial in aesthetic areas in order to improve the blend between tooth and restorative material at the margin. This is created using a modified bevel with a large round diamond bur. Illustration to follow.
Rule of BULL
Buccal cusps of Uppers and Lingual cusps of Lowers are more likely to crack. There is no cusp-fossa relationship in their envelope of function and therefore they are under tension rather than compression. For this reason, tension cusps should be onlayed if thickness <3 mm.
Overlay or Onlay?
There are many different approaches to non-retentive, adhesive preparation designs. The 2018 paper by Politano et al. referenced below shows several examples, as well as the 2017 paper by Ferraris. Most preparations are relatively flat compared to traditional preparations, with smooth and rounded internal line angles. Thick cusps should be preserved in order to maximise the fracture resistance of the tooth.
If cusps that are too thick (>3.5 mm) are onlayed, this can increase the risk of catastrophic failure. This was shown in the research by Fennis et al. in 2004, who recommended that the placement of fibre in the dentin replacement layer can reduce this risk.
Preserving the BioRim and the Compression Dome Concept
The BioRim is defined as the 2-3 mm of tooth structure (enamel, DEJ/DEC and superficial dentin) located above the CEJ.

Photo credit: Dr Steven Schiffenhaus
Enamel is said to act as a compression dome, helping to transmit compressive forces to dentin when a load is applied, and therefore reducing potentially damaging or catastrophic tensile forces. The BioRim can be described as the base of the compression dome. By removing the BioRim (e.g. by carrying out a traditional crown preparation), the compression dome is disrupted and compressive forces directed from the occlusal portion of the tooth can result in damaging tensile forces in the cervical area.
You may see the coronal portion of the tooth referred to as the BioDome. For most indirect Biomimetic restorations, the BioDome takes the form of a ceramic onlay or overlay which is adhesively bonded to the preserved BioRim. A smooth preparation allows the restoration and tooth to function well together in compression. Sharp corners or line angles should be avoided in order to minimise the potentially catastrophic concentration of forces in these areas. Standard engineering concepts should always be considered when restoring a tooth biomimetically.

Photo credit: Dr Steven Schiffenhaus
Bonding Enamel Replacement to the Biobase
As per the previous lessons in the Six Lessons Approach to Biomimetic Restorative Dentistry, the Peripheral Seal Zone (PSZ) should be achieved using appropriate Caries Removal Endpoints (CRE) and Crack Removal Endpoints (CrRE). Once onlay preparation is carried out, Immediate Dentin Sealing (IDS) and Resin Coating (RC) should be performed, and 1 mm of fibre-reinforced composite placed. Together with Deep Margin Elevation (DME), these elements form the Biobase.
After fabrication of an indirect or semi-direct restoration, the next step is to follow gold-standard adhesive protocols in order to bond to the aforementioned Biobase.
As we are bonding to previously cured composite, the surface of the composite must be treated before bonding. Air Abrasion (AA) or Air Particle Abrasion (APA) can be used to expose unreacted double bonds within the composite surface structure. This gives the potential for a strong chemical bond to form between the composite resin Biobase and the composite resin-based cement, which is commonly heated restorative composite (e.g. heated AP-X from Kuraray). The resin cement is therefore also bonded to the indirect or semi-direct composite or ceramic enamel replacement at this same stage.
Example of Bonding Protocol
Bonding protocol depends on the materials used and the type of tooth/composite structure being bonded to. An example bonding protocol is described below.
- Gold standard isolation protocol using rubber dam
- Air Abrasion of the Biobase using 29 micron Aluminium Oxide powder particles
- Application of 37% phosphoric acid for 30 seconds. Rinse for the same amount of time and then air dry
- Surface treatment of the indirect/semi-direct restoration:
- Composite: Air Abrasion followed by 37% phosphoric acid for 30 seconds. Rinse and dry
- Ceramic emax restoration: Suitable surface treatment using Hydrofluoric acid, phosphoric acid, silanisation
- Uncured adhesive is placed on the Biobase and the intaglio surface of the indirect/semi-direct restoration. As per previous steps in fabrication of the Biobase, gold standard bonding agents such as Optibond FL or Clearfil SE Protect are recommended
- Cementation using heated restorative composite (e.g. AP-X)
- Before curing, removal of excess resin cement using floss, PTFE tape, plastic instruments, brushes. After curing, any remaining excess can be removed using a number 12 blade or scaler.
Cementation Using Heated Restorative Composite
In the example protocol above, heated restorative composite is used to ‘cement’ the bonded indirect restoration. Benefits of using heated composite instead of dual-cure resin cement include:
- As the composite is light-cured on command, this allows as much time as necessary to ensure that the indirect restoration is correctly seated and all excess is removed.
- The process of removing excess is much more predictable as the composite is in a consistency which allows easy removal with plastic instruments, PTFE or floss.
- Improved mechanical and physical properties, including increased wear resistance when compared to resin cements.
- As per the study by Gregor at al., appropriate levels of polymerization can be achieved even through thick ceramic restorations. A robust light-curing protocol should be followed and each surface of the restoration should be light-cured for an appropriate amount of time (90 seconds per surface is suggested – consider alternating between each surface to avoid overheating).
As with all techniques, if using heated restorative composite to bond an indirect restoration, it is important to consider the possible limitations:
- The type of filler particle should be considered – micro-hybrid composites are generally recommended.
- The degree of viscosity achieved upon heating can vary between different brands of composite, and some composites may not achieve the desired viscosity for cementation.
- The composite heating device should be able to heat the composite to an accurate, reliable temperature and allow this temperature to be maintained – 68 degrees Celsius for 10 minutes is generally recommended.
- Some composites may cool rapidly upon removal from the heating device, and the viscosity may therefore increase to an unfavourable level.
- Some composites may begin to polymerize if stored in the heating device for too long.
An example of a restorative composite with favourable properties that is commonly used for heated cementation is Clearfil AP-X by Kuraray.
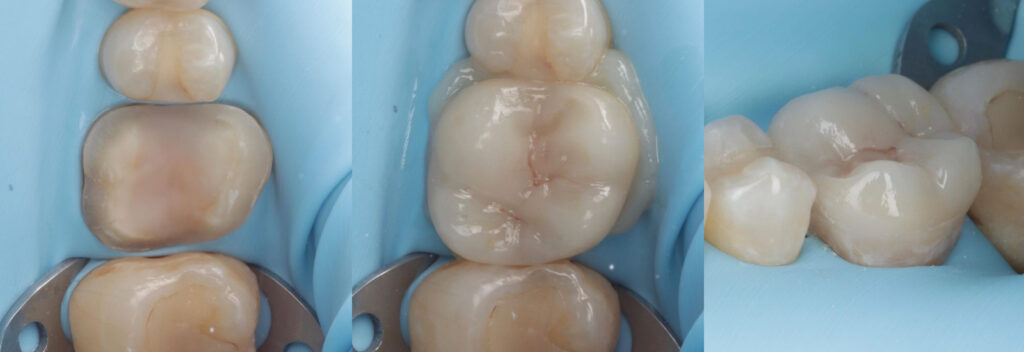
Photo credit: Dr George Cheetham
Ready to take your Biomimetic Dentistry to the next level?
Click here to access our online, on-demand Biomimetic Dentistry courses. Stay at the forefront of modern Dentistry by learning from international leaders.
Relevant Literature
Asmussen E, Peutzfeldt A. The effect of secondary curing of resin composite on the adherence of resin cement. J Adhes Dent. 2000 Winter;2(4):315-8.
Besek M, Mörmann WH, Persi C, Lutz F. Die Aushärtung von Komposit unter Cerec-Inlays [The curing of composites under Cerec inlays]. Schweiz Monatsschr Zahnmed. 1995;105(9):1123-8.
Carvalho RM, Santiago SL, Fernandes CA, Suh BI, Pashley DH. Effects of prism orientation on tensile strength of enamel. J Adhes Dent. 2000 Winter;2(4):251-7.
Fennis WM, Kuijs RH, Kreulen CM, Verdonschot N, Creugers NH. Fatigue resistance of teeth restored with cuspal-coverage composite restorations. Int J Prosthodont. 2004 May-Jun;17(3):313-7.
Fennis WM, Tezvergil A, Kuijs RH, Lassila LV, Kreulen CM, Creugers NH, Vallittu PK. In vitro fracture resistance of fiber reinforced cusp-replacing composite restorations. Dent Mater. 2005 Jun;21(6):565-72.
Ferraris F. Posterior indirect adhesive restorations (PIAR): preparation designs and adhesthetics clinical protocol. Int J Esthet Dent. 2017;12(4):482-502.
Gregor L, Bouillaguet S, Onisor I, Ardu S, Krejci I, Rocca GT. Microhardness of light- and dual-polymerizable luting resins polymerized through 7.5-mm-thick endocrowns. J Prosthet Dent. 2014 Oct;112(4):942-8.
Gresnigt MMM, Özcan M, Carvalho M, Lazari P, Cune MS, Razavi P, Magne P. Effect of luting agent on the load to failure and accelerated-fatigue resistance of lithium disilicate laminate veneers. Dent Mater. 2017 Dec;33(12):1392-1401.
Krämer N, Frankenberger R. Clinical performance of bonded leucite-reinforced glass ceramic inlays and onlays after eight years. Dent Mater. 2005 Mar;21(3):262-71.
Magne P. Immediate dentin sealing: a fundamental procedure for indirect bonded restorations. J Esthet Restor Dent. 2005;17(3):144-54; discussion 155.
Magne P, Belser UC. Rationalization of shape and related stress distribution in posterior teeth: a finite element study using nonlinear contact analysis. Int J Periodontics Restorative Dent. 2002 Oct;22(5):425-33.
Milicich G. The compression dome concept: the restorative implications. Gen Dent. 2017 Sep-Oct;65(5):55-60.
Opdam NJ, Roeters JJ, Kuijs R, Burgersdijk RC. Necessity of bevels for box only Class II composite restorations. J Prosthet Dent. 1998 Sep;80(3):274-9.
Politano G, Van Meerbeek B, Peumans M. Nonretentive Bonded Ceramic Partial Crowns: Concept and Simplified Protocol for Long-lasting Dental Restorations. J Adhes Dent. 2018;20(6):495-510.
Van den Breemer CRG, Buijs GJ, Cune MS, Özcan M, Kerdijk W, Van der Made S, Gresnigt MMM. Prospective clinical evaluation of 765 partial glass-ceramic posterior restorations luted using photo-polymerized resin composite in conjunction with immediate dentin sealing. Clin Oral Investig. 2021 Mar;25(3):1463-1473.
Wang RZ, Weiner S. Strain-structure relations in human teeth using Moiré fringes. J Biomech. 1998 Feb;31(2):135-41.